Macular degeneration is a progressive degenerative condition of the eye which causes central visual loss.
90% of macular degeneration is dry macular degeneration which causes slow progressive visual loss.
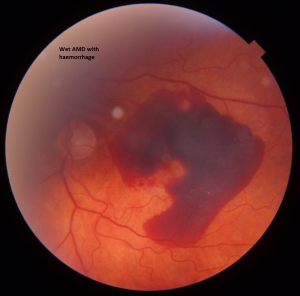
10 % of macular degeneration is wet macular degeneration, which causes rapid and significant loss of central vision leading to blindness.
Mr Saeed is an expert in macular degeneration treatments. He was the clinical lead of macular degeneration services at Epsom and St Helier NHS trust and now is a consultant in Royal Liverpool University hospital with a dedicated AMD clinic. Mr Saeed is a researcher and is the principal investigator of many macular degeneration trials.
What causes wet macular degeneration ?
Wet macular degeneration is a serious condition in which abnormal new blood vessels grow in between the layers of the retina and choroid (retina is the sensitive film at the back of the eye). These blood vessels can leak, bleed and cause scarring and water logging (called odema) in the retina. This leads to loss of vision in the area of the damaged retina. Unfortunately in most cases, this area (called macula) is responsible for central of vision. The damaged retina caused by these leaky blood vessels ultimately leads to loss of central vision.
What does wet macular degeneration cause ?
Patients suffering with wet macular degeneration may have central visual loss, blurring of vision, a grey or black patch in the centre of vision, distortion of straight lines etc. Most patients will complain of difficulty in reading.
Is treatment available ?
Treatments for this kind of eye disease have been developed in the last few years. The most effective and promising treatments for wet AMD is an injection of an anti VEGF agent. Generally speaking , there are 5 anti VEGF agents / drug classes;
1.Lucentis (Ranibizumab)
2. Avastin (Bevazicumab)
3.Eylea (Aflibercept)
4. Beovu ( Brolicizumab)
5. Vabysmo (Faricimab). ( see patient info / wet AMD choices leaflet )
Previous treatments for this eye disease were either not very effective or were very expensive. However some patients may benefit from special types of laser treatment called Argon laser, photodynamic treatment with laser treatment or even extensive laser surgery called vitreo retinal surgery.
Intravitreal injections of lucentis are now routinely given to try and stabilize vision and preserve as much vision as we can. The damage in the retina may be reduced by the injections but not totally reversed. Visual loss will be expected but hopefully not as much if the eye was not treated at all.
What tests will I need?
You will have tests which include a colour photograph of the retina, a dye test and a scan of the retina. If there are signs of wet macular degeneration that are expected to benefit from treatment, then you will have 3 injections of lucentis treatment (one injection each month for 3 months). The patient then enters an observation period and will then be offered treatment only if it is required.
What does the treatment involve?
This injection is given directly into the eye (in the jelly of the eye), by Mr Saeed. The eye will be sore for a while and the vision will be blurred for a period of time after which it will clear to previous levels.
What treatments can I have ?
You may choose to have Lucentis , Avastin or Eylea treatment.
Lucentis is licensed for macular degeneration and works extremely well.
Avastin is not licensed for macular degeneration but extensive evidence suggests that it works almost as well as Lucentis. There may be a slightly higher risk of infection due to injection preparation issues. This injection is significantly cheaper than Lucentis or Eylea. Most people wanting private treatment choose Eyle or Avastin.
Eylea is licensed for wet macular degeneration and can be given privately. This injection may require less injections than Lucentis on a year on year basis.
How many injections will I need ?
You may require at least 3-4 injections of anti VEGF agents. ( Lucentis, Eylea, Avastin, Beovu or Vabysmo). Most people will require 7 injections in the first year and 5 in the second year to keep the vision stable. However, this depends upon the sub-type of macular degeneration and the response to the drug. Some people will just require 3 injections and will become stable. Others may require over 40 injections over 4-5 years.
Am I likely to have problems?
In most cases, patients do not have any problems after the injection. Sometimes the front surface of the eye can get scratched (corneal abrasion), which can cause eye pain but settles down in a day. Occasionally people can get a cataract or retinal problems. Inflammation, bleeding or cataract can be complications after intravitreal injection treatment.
Rarely patients can get an infection in the eye that has received an injection. If the infection gets into the jelly of the eye, called endophthalmitis, it can cause total loss of vision.
Will the injection treatment work ?
The injection is likely to work in 80-90 % of people. Unfortunately it means that 10-20 % of patients will not benefit from this injection.
What can I expect?
The main benefit is likely to be stabilization of vision. This means that you may not lose more vision. In some patients the vision may improve approximately 20% of patients.
How many injections has Mr Saeed done
Mr Saeed is very experienced having given more than 1000 intra-vitreal injections over the last few years. In his experience, complications are rare but do occasionally happen.
Leaflets regarding wet and dry macular degeneration can be found in the patient info section.